Massive proximal humeral bone loss (MPHBL) remains one of the most complex and frustrating challenges in shoulder arthroplasty. When proximal humeral bone stock is severely compromised, surgeons must balance mechanical stability, soft tissue function, and long-term durability, commonly in patients who have already undergone multiple failed procedures.
A recent comparative study examining the reverse humeral reconstruction prosthesis (RHRP) from Advita Ortho, LLC versus reverse allograft–prosthetic composite (RAPC) provides deeper insight into how modern prosthetic systems are reshaping the landscape of multiple-revision shoulder arthroplasties with proximal humeral bone loss.
The Core Challenge: Rebuilding a Functional Shoulder
Successful shoulder arthroplasty depends heavily on intact proximal humeral bone. Without proximal humeral bone, surgeons lose reliable implant fixation including adequate rotational stability and critical soft tissue attachment sites. This is where proximal humeral reconstruction strategies come into play. Traditionally, allograft–prosthetic composites have been used to restore bone stock and enable soft tissue integration. However, these come with well-documented risks such as graft resorption and nonunion which can lead to implant and/or construct failure. The humeral reconstruction prostheses takes a different approach by prioritizing mechanical reliability and intraoperative flexibility over biological incorporation.
What the Study Shows:
This retrospective series of 30 patients with procedures performed between 2018 and 2024 compared RHRP (20 patients) and RAPC (10 patients), with an average follow-up of three years and an average age of 73.6 years. Most cases (93%) were complex revision surgeries, underscoring the severity of pathology that was addressed in this cohort.
Both groups improved significantly, however RHRP patients generally performed better in their final range of motion including forward flexion (110° vs. 92°) and external rotation (22° versus 12°). Similarly, the RHRP patient had better gains in range of motion including an improvement in forward flexion of 44° compared to 27° in the RAPC patients. A higher percentage of RHRP patients achieved minimal clinically important difference (MCID) across range of motion parameters. Additionally, higher Simple Shoulder Test scores (7.5 vs. 6.3) were seen in the RHRP group, with similar functional improvements noted in the Constant and VAS Pain scores between the two groups.
Clinical Outcomes Summary: RHRP vs. RAPC
| Category | Metric / Outcome Measure | RHRP Cohort (n=20) | RAPC Cohort (n=10) |
|---|---|---|---|
| Demographics | Average Age / Follow-up | 73.6 years / 3 years | 73.6 years / 3 years |
| Complex Revision Rate | 93% | 93% | |
| Range of Motion | Final Forward Flexion | 110° | 92° |
| Forward Flexion Net Gain | 44° | 27° | |
| Final External Rotation | 22° | 12° | |
| Functional Scores | Simple Shoulder Test (SST) | 7.5 | 6.3 |
| MCID Achievement Rate | Higher % | Lower % |
The difference in complications noted is hard to ignore as the RHRP cohort had a 5% complication rate compared to a 50% complication rate in the RAPC group. Complications in RAPC included instability, infection, recurrent dislocations, and one radial nerve palsy while the RHRP group had just one patient with a complication which was an infection accompanied by instability. Revision rates followed a similar pattern, with 5% in the RHRP cohort versus 50% in the RAPC cohort. This corresponded to nearly a 19-fold increased odds of revision in patients undergoing RAPC reconstruction, indicating a substantially higher risk profile in this series.
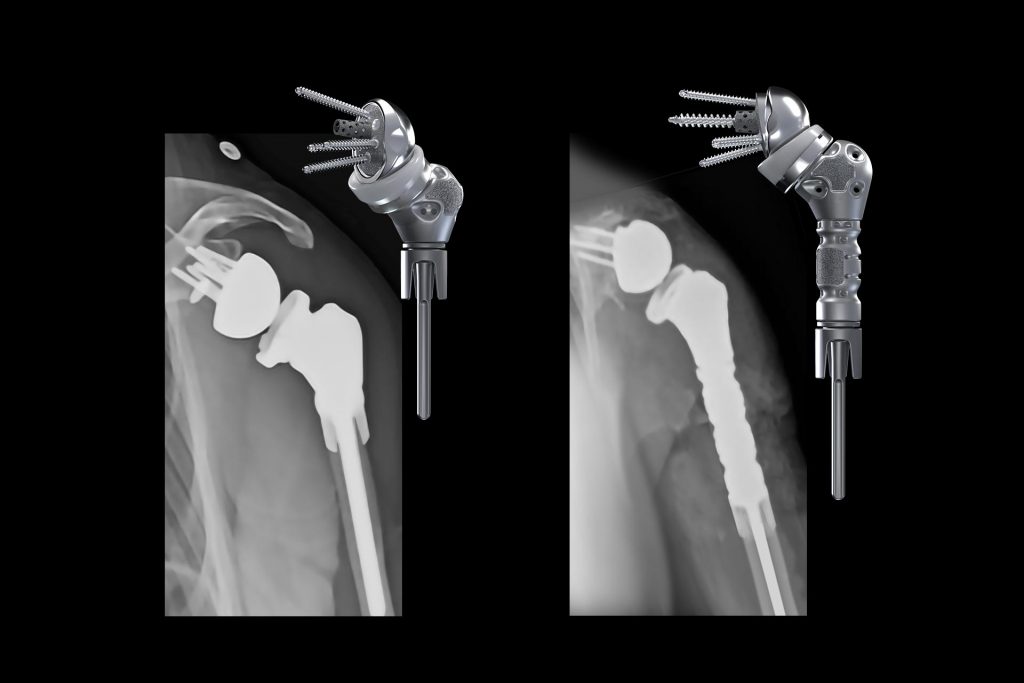
The observed differences may, in part, relate to implant design characteristics. The humeral reconstruction prosthesis used in this study allows intraoperative adjustment of humeral length across a range of 50–222.5 mm, with modular components assembled in 12.5 mm increments. The reconstruction options in this system facilitate patient-specific reconstruction and intraoperative optimization of soft tissue tensioning and deltoid wrapping. The system also incorporates a novel press-fit collar for rotational control and a cemented stem for axial stability, along with multiple options for soft tissue reattachment. While these features are designed to improve construct stability and biomechanics, this study was not structured to isolate their independent contribution to clinical outcomes, and any causal relationship should be interpreted cautiously.
Analysis using the PHAROS classification system demonstrated that the severity of proximal humeral bone loss was not an independent predictor of postoperative forward flexion. Instead, preoperative forward flexion was significantly associated with postoperative outcomes (P = .008), whereas PHAROS classification was not (P = .620). When stratified by PHAROS Type 2 and Type 3 bone loss, both groups achieved comparable improvements in range of motion and patient-reported outcomes, despite differences in absolute postoperative values. These findings suggest that, within the limits of this small dataset, the degree of bone loss alone does not dictate clinical improvement following reconstruction.
Radiographic outcomes were similarly reassuring in both cohorts. No evidence of humeral component loosening, migration, or subsidence was observed in the RHRP group. In the RAPC cohort, all cases demonstrated graft–host union without evidence of nonunion, graft resorption, or periprosthetic fracture. These findings indicate that both techniques can achieve short- to mid-term radiographic stability. While another study looking at 44 RHRPs with minimum 2-year follow-up noted no humeral loosening as well1, other studies have noted significant humeral-sided complications with RAPCs.2,3 One study looking at another reverse endoprosthesis noted aseptic humeral loosening rates of 22% in revision shoulder arthroplasty and a total humeral loosening rate of 11% in all of the 53 patients studied including primary and revision arthroplasty.4 These studies along with the current study suggest a much lower humeral-sided complication rate with the RHRP implant.
These results are broadly consistent with prior literature evaluating reconstruction in the setting of massive proximal humeral bone loss. Reverse total shoulder arthroplasty has been shown to provide more reliable pain relief and functional improvement than anatomic constructs or hemiarthroplasty in this population, largely due to its ability to compensate for rotator cuff deficiency and restore deltoid-driven mechanics. However, instability remains a recognized complication, particularly in the setting of substantial proximal humeral bone loss and compromised soft tissue tensioning.5,6 In this context, both the current study and prior reports highlight the importance of restoring humeral length and optimizing soft tissue balance.
Comparative data from a meta-analysis by Hao et al.5, which included 18 articles comparing 267 reverse APC and 260 reverse endoprostheses with mixed indications (including oncologic indications), demonstrated that both RAPC and humeral reconstruction prostheses can achieve comparable forward elevation and patient-reported outcomes. However, complication profiles vary across studies. Revision surgery rates were higher for RAPCs in this meta-analysis (12%) compared to 7% in the endoprosthesis cohort, but this was a much lower rate of revision surgery for RAPCs than was noted in the current study. Dislocation was the most frequently reported complication across studies, reinforcing the importance of implant selection and soft tissue management in these complex reconstructions. Another study of 14 RAPCs for MPHBL had a 43% complication rate, of which all required revision.7
Limitations:
Several limitations should be acknowledged. This study is retrospective, with a relatively small sample size, particularly in the RAPC group, limiting statistical power and increasing susceptibility to type II error. Treatment allocation was influenced by insurance approval, introducing potential selection bias. Additionally, variability in surgical indications and the absence of subscapularis repair in both groups may have influenced stability and functional outcomes.
Conclusion:
In summary, both RHRP and RAPC provided meaningful clinical and radiographic improvement in patients with massive proximal humeral bone loss. Within the limitations of this study, RHRP was associated with greater forward flexion, higher Simple Shoulder Test scores, and substantially lower rates of complications and revision. Outcomes were not independently determined by the severity of bone loss as classified by PHAROS. These findings support the role of humeral reconstruction prostheses as a viable reconstructive option, while underscoring the need for larger, prospective comparative studies to better define optimal surgical indications and techniques.
References:
- Srinivasan RC, Wright JO, Hao KA, King JJ, Schoch BS, Farmer KW, et al. Two-year outcomes of the reverse humeral reconstruction prosthesis. J Shoulder Elbow Surg. 2023;32: S75—84. https://doi.org/10.1016/j.jse.2023.01.022.
- Cox JL, McLendon PB, Christmas KN, Simon P, Mighell MA, Frankle MA. Clinical outcomes following reverse shoulder arthroplasty-allograft composite for revision of failed arthroplasty associated with proximal humeral bone deficiency: 2- to 15-year follow-up. J Shoulder Elbow Surg. 2019 May;28(5):900-907. doi: 10.1016/j.jse.2018.10.023.
- Rampam S, Segu H, Gonzalez MR, Lozano-Calderon SA. Complications and functional outcomes after reconstruction of the proximal humerus with allograft-prosthetic Composite—A systematic review of the literature. J Shoulder Elbow Surg. 2024;10:1873—83. https://doi.org/10.1016/j.jse.2024.02.037.
- Labrum JT IV, de Marinis R, Atwan Y, Marigi EM, Houdek MT, Barlow JD, et al. Reverse shoulder arthroplasty megaprosthesis for surgical management of severe proximal humeral bone loss. J Shoulder Elbow Surg. 2024;33:S64—73. https://doi.org/10.1016/j.jse.2023.12.020.
- Hao KA, Gutowski CT, Bindi VE, Srinivasan RC, Wright JO, King JJ, Wright TW, Fedorka CJ, Schoch BS, Hones KM. Reverse Allograft Prosthetic-Composite Versus Endoprosthesis Reconstruction for Massive Proximal Humerus Bone Loss: A Systematic Review and Meta-analysis of Outcomes and Complications. Indian J Orthop. 2024 Sep 1;58(10):1339-1348. doi: 10.1007/s43465-024-01248-7.
- Kany J, Jose J, Katz D, Werthel JD, Sekaran P, Amaravathi RS, et al. The main cause of instability after unconstrained shoulder prosthesis is soft tissue deficiency. J Shoulder Elbow Surg. 2017;26:e243—51. https://doi.org/10.1016/j.jse.2017.01.019.
- Cox RM, Mandava N, Lazarus MD, Williams GR Jr., Namdari S. Management of proximal humerus bone loss with allograft prosthetic composite technique in shoulder arthroplasty. J Shoulder Elbow Surg. 2024;33:1306—12. https://doi.org/10.1016/j.jse.2023.09.038.